Page 3 - Surgery #2 - Curvature Correction And Instrumentation
 Curvature of the spine, or scoliosis, can be caused by congenital, developmental or degenerative problems. However, at present, the vast majority of cases of scoliosis actually have no known cause.
Curvature of the spine, or scoliosis, can be caused by congenital, developmental or degenerative problems. However, at present, the vast majority of cases of scoliosis actually have no known cause.
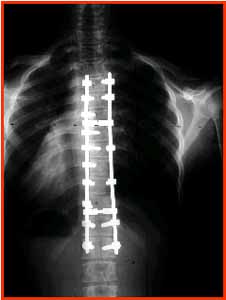
An 11 hour operation resulted in Sue's back being returned to an "S" instead of a "C" and the rotation from 50 degrees to approximately 14 degrees!!!!!
It is important to note that scoliosis is not usually a cause of back pain. The condition represents a deformity of the spine but is not usually painful. Of course, people with scoliosis can develop back pain, just as most of the adult population can develop back pain. However, it has never been found that people with idiopathic scoliosis (the most common form of scoliosis) are any more likely to develop back pain than the rest of the population. People with degenerative scoliosis can develop pain from osteoarthritic joints.
Scoliosis usually develops in the thoracic spine (upper back) or the thoracolumbar area of the spine, which is between the thoracic spine and lumbar spine (lower back). It may also occur just in the lower back. The curvature of the spine from scoliosis may develop as a single curve (shaped like the letter C) or as two curves (shaped like the letter S).
Scoliosis Surgery
 For those who cannot stay functional despite aggressive conservative treatment, surgery may be considered. In Sue's case, surgery was mandatory.
For those who cannot stay functional despite aggressive conservative treatment, surgery may be considered. In Sue's case, surgery was mandatory.
Most patients will not need surgery for their scoliosis, as the curves tend to either not progress or to progress at a very slow rate. The progression is typically no more than 1 to 3 degrees per year, so it takes many years of observation to see any significant progression of the curve in an adult.
Also, because the curve is in the lumbar spine, progression of the curve is very unlikely to influence the lungs or heart (as it would in the thoracic spine).
Therefore, unlike surgery for idiopathic scoliosis, the goal of surgery for degenerative scoliosis is not to prevent deformity as much as it is to treat pain.
Seeing The Screws
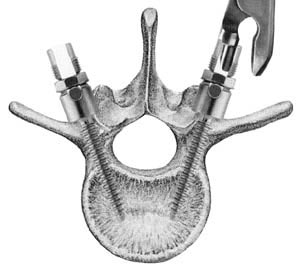
Spinal fusion
is the most widely performed surgery for scoliosis. In this procedure, bone (either harvested from elsewhere in the body (autograft), or donor bone (allograft) is
grafted
to the vertebrae so that when it heals, they will form one solid bone mass and the
vertebral column
becomes rigid.
This prevents worsening of the curve at the expense of spinal movement.
This can be performed from the anterior (front) aspect of the spine by entering the
thoracic
or
abdominal cavity
, or performed from the back (posterior). A combination of both is used in more severe cases.
Xrays
 Originally, spinal fusions were done without metal implants. A
cast
was applied after the surgery, usually under
traction
to pull the curve as straight as possible and then hold it there while fusion took place. Unfortunately, there was a relatively high risk of
pseudarthrosis
(fusion failure) at one or more levels and significant correction could not always be achieved. In 1962, Paul Harrington introduced a metal spinal system of instrumentation which assisted with straightening the spine, as well as holding it rigid while fusion took place. The original, now obsolete
Harrington rod
operated on a ratchet system, attached by hooks to the spine at the top and bottom of the curvature that when cranked would distract, or straighten, the curve. A major shortcoming of the Harrington method was that it failed to produce a posture where the skull would be in proper alignment with the pelvis and it didn't address rotational deformity. As a result, unfused parts of the spine would try to compensate for this in the effort to "stand up straight".
Originally, spinal fusions were done without metal implants. A
cast
was applied after the surgery, usually under
traction
to pull the curve as straight as possible and then hold it there while fusion took place. Unfortunately, there was a relatively high risk of
pseudarthrosis
(fusion failure) at one or more levels and significant correction could not always be achieved. In 1962, Paul Harrington introduced a metal spinal system of instrumentation which assisted with straightening the spine, as well as holding it rigid while fusion took place. The original, now obsolete
Harrington rod
operated on a ratchet system, attached by hooks to the spine at the top and bottom of the curvature that when cranked would distract, or straighten, the curve. A major shortcoming of the Harrington method was that it failed to produce a posture where the skull would be in proper alignment with the pelvis and it didn't address rotational deformity. As a result, unfused parts of the spine would try to compensate for this in the effort to "stand up straight".
As the person aged, there would be increased "wear and tear", early onset arthritis, disc degeneration, muscular stiffness and pain with eventual reliance on painkillers, further surgery, inability to work full-time and disability. "Flatback" became the medical name for a related complication, especially for those who had lumbar scoliosis.Modern spinal systems are attempting to address
sagittal
imbalance and rotational defects unresolved by the Harrington rod system. They involve a combination of rods, screws, hooks and wires fixing the spine and can apply stronger, safer forces to the spine than the Harrington rod. Spinal fusion is rarely performed without this instrumentation.